Scolioses at different age groups
It has been suggested that scolioses be classified by their age groups in which they were diagnosed because:
1. In majority of cases, the causes can not be identified, hence they are known as idiopathic (unknown), and
2. Age of diagnosis is significant as it has been observed the longer the period between diagnosis and completion of growth of the child, the greater the likelihood of a more severe deformity.
{kind=link}
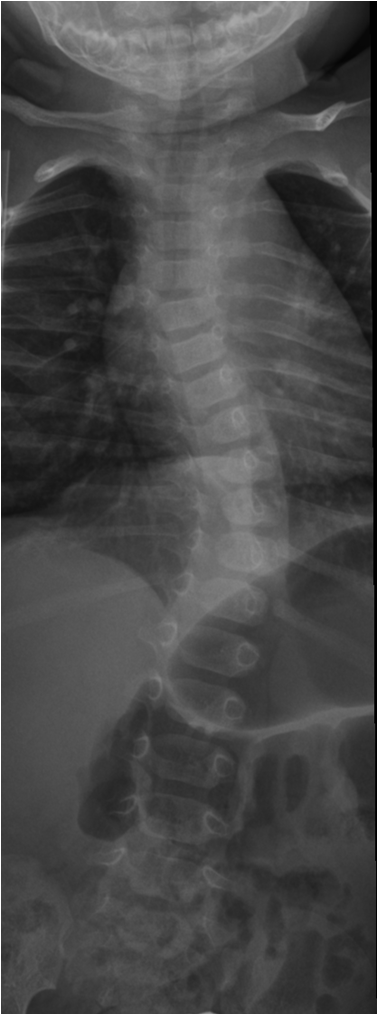
Infantile Scoliosis (0-2)
Infantile scoliosis is a scoliosis diagnosed in children under two years of age. Unlike scoliosis in adolescents and adults, scoliosis in infants and young children has more identifiable causes, including congenital or developmental abnormalities, neuromuscular diseases, and some are unknown.
What causes infantile scoliosis?
Congenital anomalies: Some babies are born with spinal abnormalities that make them prone to scoliosis. Abnormal development of the spinal structures in the womb, can cause noticeable curvatures within first years of birth.
Neuromuscular Diseases: Conditions that affect the nerves and muscles can cause scoliosis in babies. Diseases such as cerebral palsy or muscular dystrophy may affect the control and balance of muscle tone, causing uneven tension on the spine, leading to scoliosis.
Unknown: In a significant number of cases, the exact cause of infantile scoliosis is unknown (classified as idiopathic). The lack of a clear cause makes diagnosis and treatment difficult, however, this also highlights the importance of vigilant monitoring in early childhood.
Treatment options for infantile scoliosis
Causes can be identified more in infantile scoliosis more than other ages groups. While many underlying causes can not be cured, the treatment is targeted towards addressing the underlying cause where possible, and also improving function and preventing future disability.
{kind=link}
Juvenile Scoliosis (3-9)
Juvenile scoliosis is a form of idiopathic scoliosis that affects children aged 3 to 9 years. In this age group, other than idiopathic (of unknown cause) scoliosis, paediatricians and family doctors normally would have identified spinal abnormalities due to common causes.
Juvenile scoliosis is more common in girls than boys. Among children aged 3 to 6 years, the ratios are about equal between boys and girls. However, the incidence is higher among girls between the ages of 6 and 9 years.
An estimated 70% of children diagnosed with juvenile scoliosis are likely to worsen and require proactive monitoring and support and many require surgery.
What causes juvenile scoliosis?
Juvenile scoliosis has similar clinical features to adolescent scoliosis. This has led to juvenile idiopathic scoliosis sometimes being labelled as an early onset adolescent idiopathic scoliosis.
How is juvenile scoliosis diagnosed?
Juvenile idiopathic scoliosis is usually first suspected by the parents of a child, who may notice uneven shoulders or hips.
A common test used by health professionals to screen for scoliosis is the Adams forward bending test. In this test the child bends forward at the waist, and the examiner observes for the presence of a rib hump or spinal asymmetry. You can see how it is done and how to screen your child by following this link. An X-ray may be necessary to confirm diagnosis.
Mild scoliosis does not typically cause significant pain in children. However some discomfort and stiffness are not uncommon. If a scoliosis is suspected a comprehensive physical examination should be carried out, and depending on the results, an X-ray or MRI may be needed to rule out medical conditions that potentially cause or contribute to spinal deformity.
Treatment options for juvenile scoliosis
Treatment pathways are similar to adolescent idiopathic scoliosis (AIS). Please read the below section for details.
{kind=link}
Adolescent Idiopathic Scoliosis (10-17)
Children with adolescent idiopathic scoliosis (AIS) are generally healthy. About 3% of children ages 10 to 18 develop AIS, and AIS is around 80% of all scolioses. AIS is more common in girls than boys.
AIS can develop into severe deformity if not detected early and treated appropriately. It is not uncommon for teenagers with significant curves which progress from an initially mild curve within months.
What causes AIS?
The cause of AIS is unknown, hence it is classified as an idiopathic (unknown or unexplained) scoliosis. AIS is common among members of the same family, the same generation, and prior generations. Current theories suggest that genetics play a significant role and the onset may be triggered by hormonal or environmental cues.
Treatment options for AIS
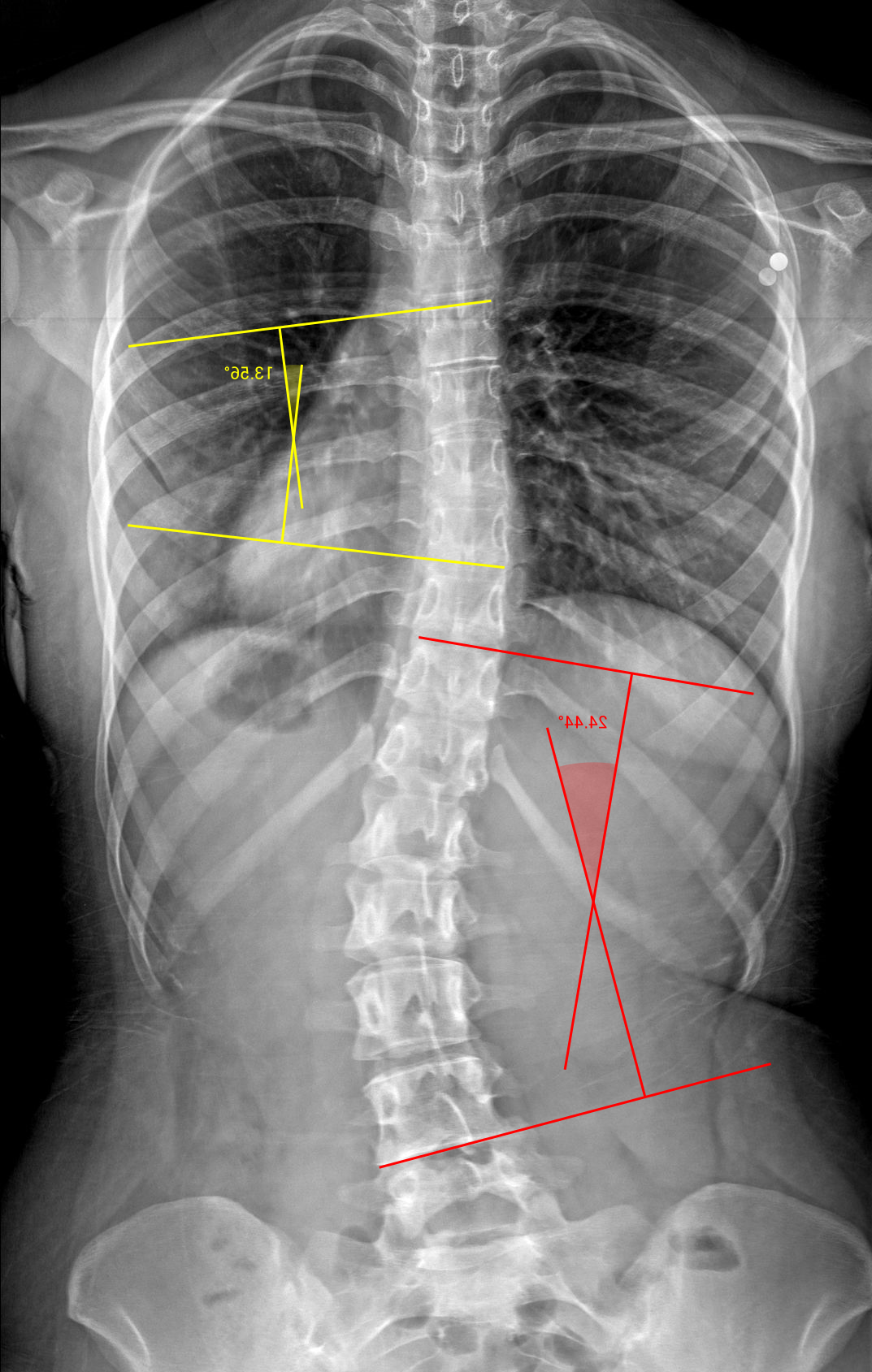
Exercise Rehabilitation – In mild to moderate curves between 10 and 20 degrees there is some evidence that an intensive course of scoliosis specific exercises may be able to make some correction or control the curve. However once the curve is greater than 20 degrees, bracing is added to exercises.
Bracing – In curves greater than 20 degrees, bracing is usually recommended. Scoliosis specific exercises is often prescribed to complement bracing to continue active correction and maintain muscle strength, and to counter some of the deleterious effect of immobilisation. AIS between 20-45 degrees, the treatment is typically a combination of scoliosis specific exercises and bracing
Surgery – In curves greater than 45 degrees, surgery may be required to control progression. The decision depends on the goal (e.g. to stop curve progression), and also whether the child has reached skeletal maturity. If not, a rigid brace and intensive physiotherapy may be recommended to stabilise the curve until the patient is mature and ready for surgery. Whereas in an older adolescent even with a significant curve, if there is reasonable spinal balance, surgery may not be necessary as the likelihood of progression is not as high.
{kind=link}
Adult Scoliosis (18+)
What causes adult scoliosis?
1. It evolved from Adolescent Idiopathic Scoliosis (AIS). This is called Adolescent Scoliosis in Adults (ASA). Curve progression can be monitored by regular physical examination and comparing current X-rays with X-rays taken during adolescence.
2. It is caused by spinal degeneration. This is called Degenerative de-novo Scoliosis (DDS). DDS usually occurs in middle-aged and older adults. Because DDS is caused by degeneration of spinal joints and tissues, leading to instability and compensation. DDS is usually progressive if not treated.
Pain and scoliosis in adults
Pain is a significant cause of impairment and disability in adult scoliosis.
A common misconception held by many health professionals is that scoliosis does not cause pain. The idea that there is no pain associated with scolioses comes about because most children scoliosis during development do not present with pain as their chief complaint. This misunderstanding has led to therapeutic approaches that largely ignore the progressive nature of pain associated with abnormal loading and degenerative changes in adult scolioses, and not take sufficiently early and proactive steps to address the symptoms.
Treatment options for adult scoliosis
It is not uncommon for adults with scoliosis to experience pain, due to the accelerated wear-and-tear related to asymmetric loading. Therefore, it makes sense to consider bracing in patients with unstable spine, and recommend specific exercises to improve flexibility in some areas and stabilise other areas to prevent onset of symptoms and disability.