How often do I need new X-rays?
For adolescents, the frequency may range between every 3-12 months depending upon initial curve severity, age of discovery, expected curve progression, and skeletal maturity (Risser Sign). For adults with scoliosis, less frequent monitoring is required as the spine is more stable. However, if pain (especially new pain) is present, a new set of X-rays should be requested.
Will cancer risk increase due to excess radiation?
While radiation exposure is a legitimate concern, patients undergoing X-ray examination (even cumulatively) receive effective doses significantly lower in comparison with other forms of radiographic examination.
Precautions and protection
It is better to have X-rays at a facility with modern digital equipment because newer systems minimise exposure by using better detectors and software manipulation to enhance images.
Since soft tissue is more susceptible to radiation, ask the technician to provide a lead apron to shield the breasts and the ovaries/genitals where possible.
If you as a parent or patient, are highly concerned about radiation risk, look for an electro-optical sensor (EOS) imaging centre. EOS is said to offer better image quality with significantly reduced exposure when compared to conventional X-ray.
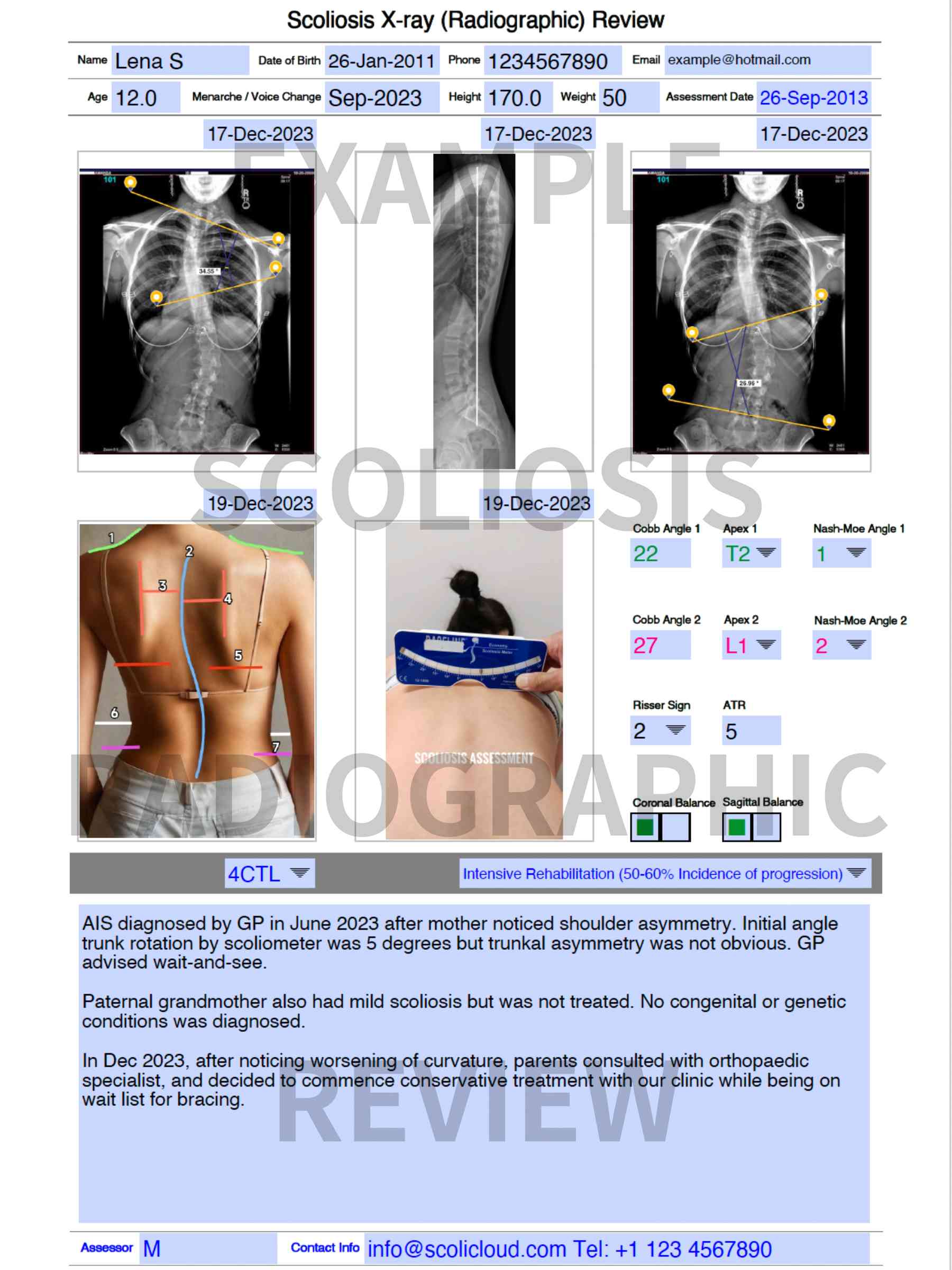
What is the likelihood of the scoliosis getting worse?
In general, the earlier the age in which scoliosis is diagnosed, the greater the Cobb angle(s) at the time of diagnosis, the greater the likelihood of a severe scoliotic curve. This is why early diagnosis and pro-active therapy (not wait-and-see!) are so important. The likelihood of curve progression can be calculated using the Lonstein formula (Karavidas NS 2016), which is part of our X-ray review.