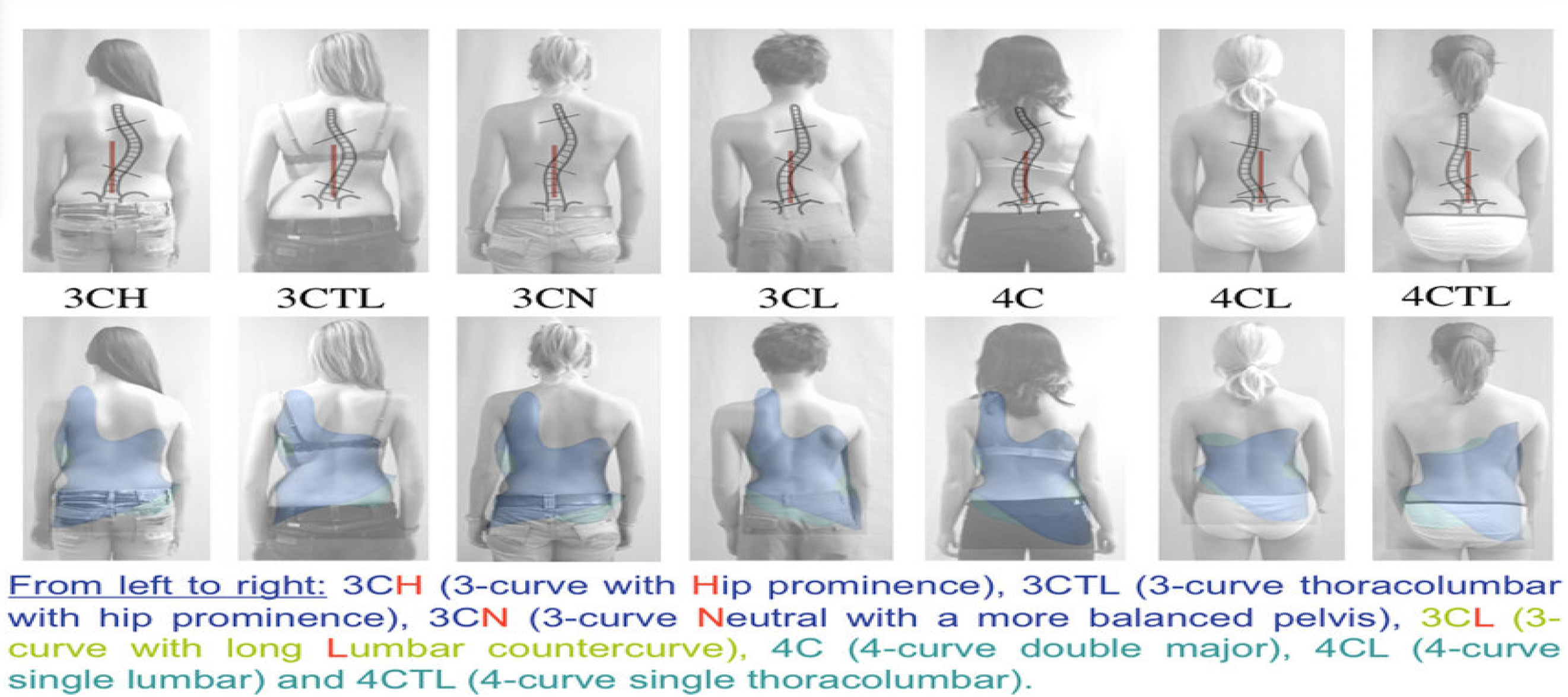
The following is an overview of the Augmented Lehnert-Schroth(ALS) Classification, a schema for scoliosis curvature named by Dr Hans-Rudolf Weiss after his mother Christina Lehnert-Schroth and grandmother, Katharina Schroth, the conceptual founders of the Schroth method.
While ALS Classification itself is continually revised and updated, many scoliosis classification systems used today were derived from or inspired by ALS Classification. In exercise-based intervention, Schroth method‘s core concept of side-shift, rotational breathing, decompression, de-tethering and de-rotation, feature prominently in various later approaches.
Click this link to read more about the remarkable 100+ years of history of the Schroth method.
3CH
3-block curve pattern with a hip prominence on the side of thoracic concavity
Clinical features
Single large primary thoracic curve
Decompensation to thoracic convex side
Long thoracic curve, no clear lumbar counter-curve
Significant hip prominence on the side of thoracic concavity, more obvious than 3CN
Weight on thoracic convex side
Radiologic features
Thoracic curve longer than lumbar curve
Thoracic Cobb angle > lumbar Cobb angle
Apex is not at thoracolumbar junction (T12/L1, otherwise consider 3CTL)
Lumbar apex does NOT cross the Central Sacral Line (CSL)
3CTL
A form of 3CH, with one long thoracolumbar curve and hip prominence on the side of thoracolumbar concavity
Clinical features
Long thoracolumbar curve with no lumbar counter curve
Hip prominence on thoracolumbar concavity
Radiologic features
Thoracolumbar curve longer than lumbar curve
Apex at T12 or L1
Thoracic Cobb angle > lumbar Cobb angle
No lumbar counter-curve
3CN
Clinical features
Thoracic curve longer than lumbar curve
Hip prominence on thoracic concavity or centred
Radiologic features
Thoracolumbar curve longer than lumbar curve
Thoracic Cobb angle > lumbar Cobb angle
Lumbar apex crosses Central Sacral Line (CSL)
Hip prominence on the thoracic concave side or balanced
3CL
Clinical features
Thoracic curve and lumbar curve similar in lengths
Hip prominence on thoracic convexity
*Clinically treated as a functional 4C
Radiologic features
Thoracic curve and lumbar curve similar in lengths
Thoracic Cobb angle > lumbar Cobb angle
Lumbar apex crosses the Central Sacral Line (CSL)
No wedging of disc space at L4/L5/S1
4C
Clinical features
Thoracic curve and lumbar curve similar in lengths
Hip prominence on thoracic convexity
Radiologic features
Thoracic curve and lumbar curve similar in lengths
Thoracic Cobb angle = lumbar Cobb angle
Lumbar apex DOES cross the Central Sacral Line
Wedging of disc space at L4/L5/S1
4CL
Clinical features
Lumbar curve with short thoracic counter curve
Hip prominence on thoracic convexity
Ventral rib hump on the side of lumbar convexity
Radiologic features
Thoracic curve and lumbar curve similar in lengths
Lumbar Cobb angle > thoracic Cobb angle
Main curve apex at L2 or below
Wedging of disc space at L5/S1
4CTL
Clinical features
Thoracolumbar curve bigger and longer than thoracic curve
Hip prominence on thoracic convexity
Ventral rib hump on the side of thoracolumbar concavity
Radiologic features
Thoracolumbar curve with short thoracic counter curve
Thoracolumbar Cobb angle > thoracic Cobb angle
Thoracolumbar curve apex at L1
Wedging of disc space at L4/L5/S1
Note on ALS Classification
Please note as the patient’s scoliosis changes with growth and exercises, his/her spinal alignment may evolve into a different pattern.
Regular follow-up examination and X-ray review by an experienced therapist are essential especially during the growth spurts, such that the prescribed exercises and bracing are continually adjusted to fit and serve the patient’s needs.